This page deals with (a) the role of the autonomic and somatic nerves in the reflex coordination of the bladder and urethral sphincters, (b) the role of the spinal cord and brainstem in the control of micturition (voiding: bladder emptying), and (c) the pathogenesis of neurogenic bladder, and of urge and stress incontinence. |
|
The bladder consists of two parts:
The smooth muscle is mainly in the dome, and is called the detrusor: its fibres extend in all directions –when it contracts it can raise bladder pressure by up to 40-60 mm Hg in men (less in women). This pressure gradient is the force that drives voiding (the expulsion of urine). The detrusor is innervated by the pelvic nerves (S2-4 in humans), which are parasympathetic nerves that initiate bladder contraction. The bladder neck consists mainly of elastic tissue and is normally closed, but opens at the start of voiding. |
The urethra is surrounded by sphincteric muscles that offer a resistance to bladder emptying, and are therefore relevant to the maintenance of continence. In the male, the prostate gland with surrounds one portion of the urethra also contributes resistance to urine flow. The Urethral Sphincters are of two types:
Pull-through manometry applied to the urethral sphincter shows the presence of a high pressure zone at the level of the prostatic urethra. The internal sphincter is also involved in male reproductive function, and ensures that semen does not pass retrogradely into the bladder during ejaculation. |
|
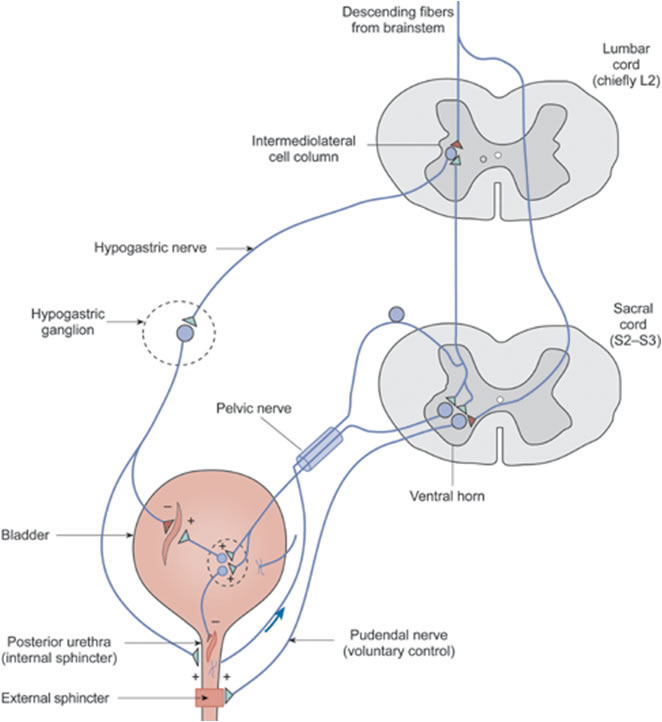
The diagram shows the innervation of the lower urinary tract. The sacral parasympathetic fibres pass towards the bladder in the pelvic nerve, synapse in the pelvic ganglia and cause the bladder to contract. Sympathetic fibres aising from the upper lumbar cord pass through the hypogastric nerve and inhibit bladder smooth muscle. Afferent fibres in the pelvic nerve monitor the volume and contractile state of the bladder, and initiate the micutition reflex. Alpha motoneurones originating in Onuf's nucleus in the ventral horn of the sacral cord innervate the skeletal muscle of the external sphincters. Coordination of these neural influences is essential for normal micturition. |
|
|
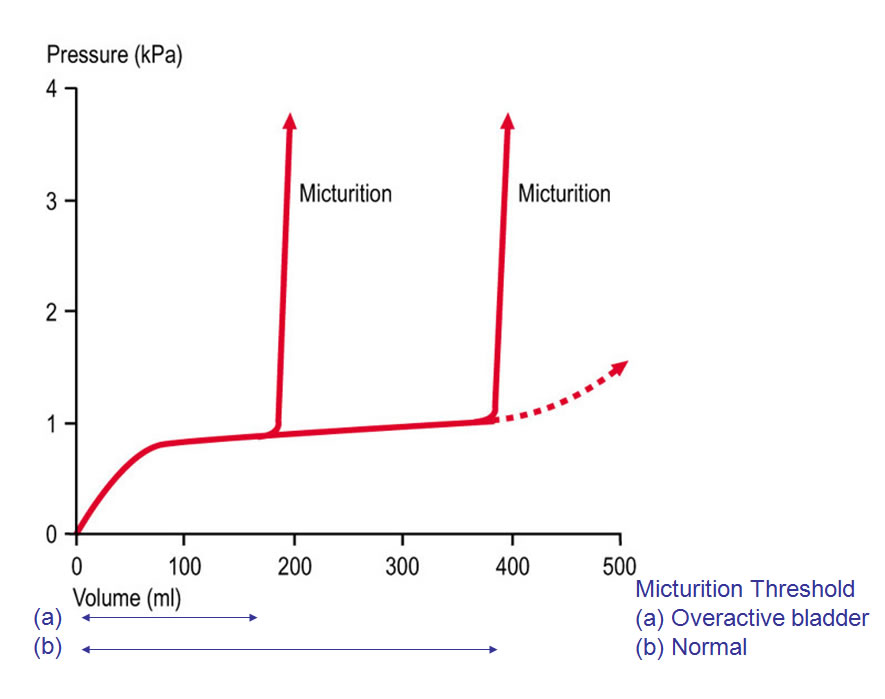
The bladder undergoes a cycle of (slow) filling followed by (rapid; voluntary) voiding. During the slow FILLING PHASE – the majority of the time- urine collects in the bladder. At this time the bladder smooth muscle is relaxed, and the sphincters contract to maintain continence. The sympathetic nerves and the relaxation of smooth muscle enhance this function. MICTURITION (Voiding) occurs once the bladder has filled to a level which is different in different individuals and also dependent on other factors. Once the bladder has filled to a certain level (the MICTURITION THRESHOLD), it begins to contract under the influence of the parasymapthetic nerves that are activated by reflex control. Bladder contraction is essential for micturition, and is under reflex and voluntary control. In both instances, the bladder contracts and there is reflex relaxation of the urethral sphincter. The Micturition Reflex is elicited by bladder distension, normally when the bladder is full. It is mediated by bladder afferents in the pelvic nerve. These sensory neurones make connections
So when the bladder contracts there is a coordinated relaxation of the urethral sphincters. Higher centres (e.g. the cerebral cortex and brainstem) can either facilitate or inhibit the micturition reflex, and provide the conscious control that is developed in infancy. | 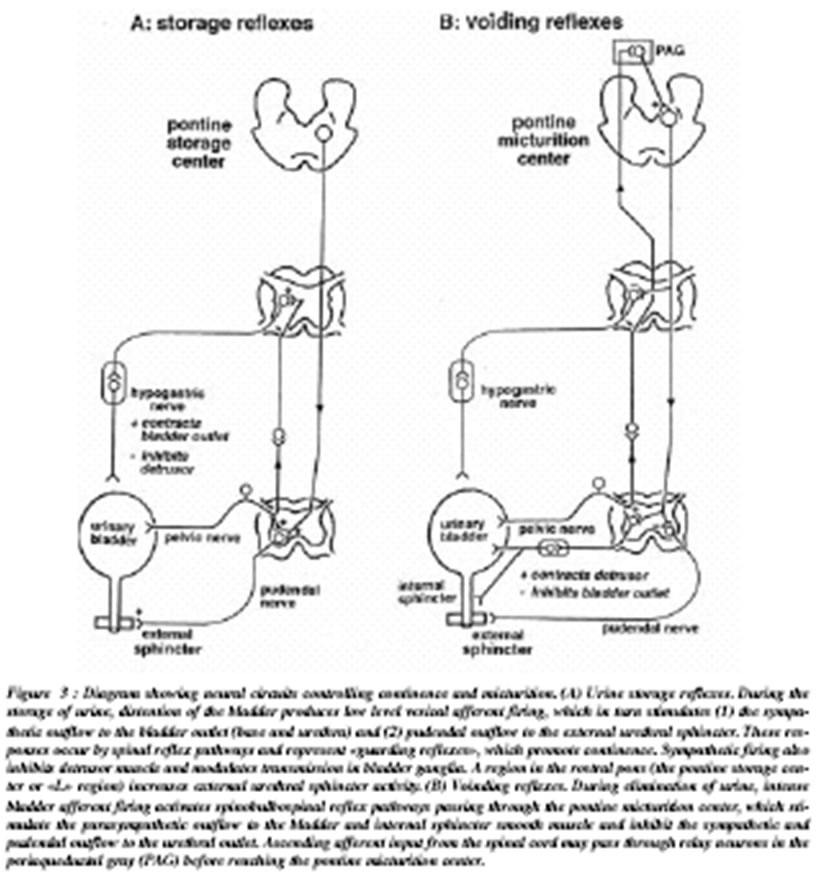
|
|
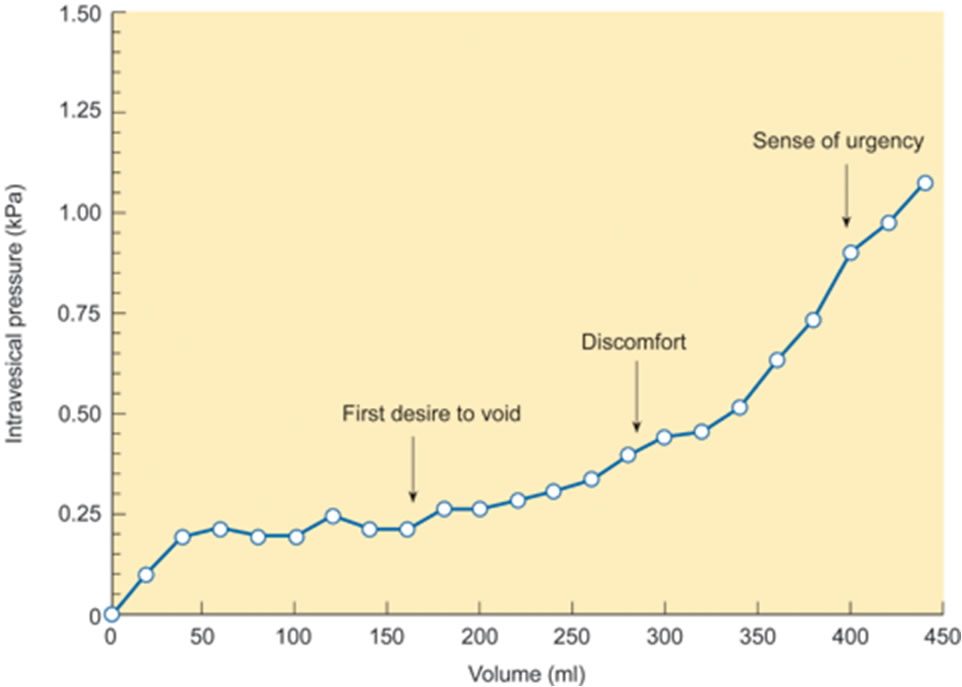
Bladder Sensation The cystometrogram is a graph of the pressure in the bladder (Y axis) obtained when the bladder is gradually distended (X axis) When the bladder is empty, the pressure is ~0. A small increase in volume causes the pressure to rise to about 10 cms H2O. A further 300 or 400 mls can accumulate without much rise in pressure (‘accommodation’), but further distension is associated with a significant rise in pressure During distension, the subject becomes aware that filling is occurring, and, later, of a ‘desire to void’ In normal life, the sensation of ‘desire to void’ can be suppressed for a while even when the bladder is full, and the micturition reflex is inhibited at this time. –The cortex and brainstem are both involved in suppression of the micturition reflex. Normally the bladder does not contract during bladder filling, but when the bladder is full, the reflex micturition contraction elevates the pressure markedly, and the sphincters relax.
|
|
|
The Cystometrogram The cystometrogram is an investigation in which the pressure in the bladder is plotted again the volume of uring in the bladder. When the bladder is empty, the pressure is ~0. A small increase in volume causes the pressure to rise to about 10 cms H2O. A further 300 or 400 mls can accumulate without much rise in pressure, but further distension is associated with a significant rise in pressure In normal life, the sensation of ‘desire to void’ can be suppressed for a while even when the bladder is full, and the micturition reflex is inhibited at this time. The cortex and brainstem are both involved in suppression of the micturition reflex. Normally the bladder does not contract during bladder filling, but when the bladder is full, the reflex micturition contraction elevates the pressure markedly, and the sphincters relax. This is known as the Overactive Bladder. |
|
|
Automatic Bladder. In patients with spinal cord transection, the bladder is atonic during the period of spinal shock, immediately after spinal cord injury, and all reflexes are depressed. In some patients a spinal reflex develops slowly after the injury (“automatic micturition”), and this is a segmental spinal reflex. In this condition, the bladder contracts when the bladder is full but the bladder never empties fully. Stimulation of the skin of the thighs or abdomen can cause the bladder to contract. | In some neurological disorders the bladder can become overactive, i.e. the bladder contracts reflexely before it is full (detrusor overactivity; hyperactive bladder). Inevitably voiding occurs frequently, and there is a sensation of desire to void at low bladder volumes. This is ‘Urge Incontinence” Damage to the peripheral nerves or to the spinal cord/brainstem or the higher centres. e.g. damage to the pudendal nerve is associated with a weak sphincteric mechanism. Because of this weakness, leakage of urine can occur during walking, laughing or coughing. This is known as “Stress Incontinence” |