|
Sensory areas
There is a general rule that one cerebral hemisphere handles sensory inputs from the opposite side of the body. This is true of the somatosensory cortex, and the visual system, where each visual area processes information relating to the opposite visual field of both eyes. The auditory cortex is an exception however, because localisation of sound requires comparison of the times of arrival of sounds at both ears; hence each auditory cortex receives inputs from both cochleas.
Sensory inputs to the cortex arise from the thalamic nuclei, including the medial and lateral geniculate bodies. There is a topographic map of one half of the body's surface on the contralateral somatosensory cortex, and a map of the contralateral visual fields of both eyes on the visual cortex. There is also a map of the cochlear basilar membranes on the auditory cortex, in keeping with the need to localise sounds.
The cortical area given over to the fovea in the primary visual cortex is much larger that than given to the peripheral retinal fields; this is a result of the fovea having an extremely dense sensory innervation, allowing finer visual definition of objects focused on the fovea. The amount of cortex involved in processing signals from the fovea is correspondingly increased. Similarly, the sites on the body surface with greatest two-point discrimination (i.e. densest innervation) have the largest areas of somatosensory cortex. The map of the body surface on the cortex is therefore distorted, depending on the density of innervation of the skin, and this distorted map is called the homonculus.
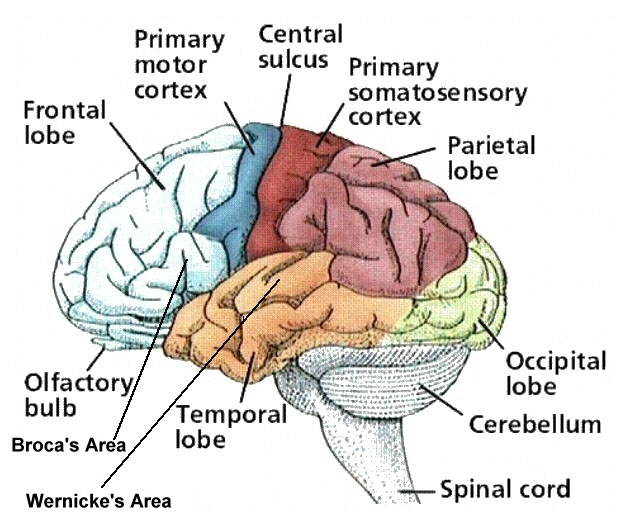
Somatosensory Cortex
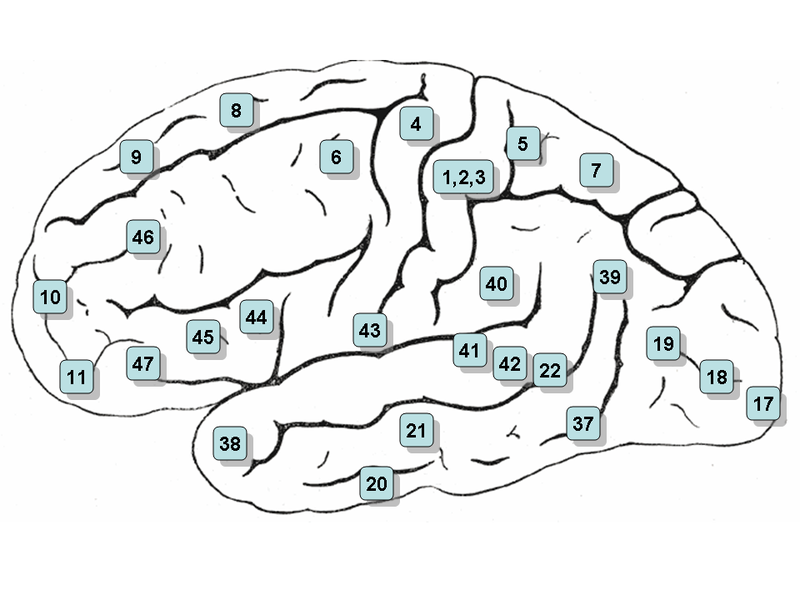
Primary somatosensory cortex (SI) is located in the post central gyrus (Brodmann's areas 1,2,3). This contains a somatotopic map, as does the thalamus, and in both structures the map of the body surface is distorted, depending on the density of sensory innervation in each part of the body. The hands, feet, genitalia and lips are the most sensitive areas (with the most dense innervation relative to the other areas) and these areas of the body surface have a relatively huge representaion on the cortex. As a result the sensory homunculus is grossly distorted with large areas of cortex given over to handling information arising in the most sensitive ares of the body. Damage to the sensory cortex results in decreased sensory thresholds, an inability to discriminate the properties of tactile stimuli or to identify objects by touch.
If a region of the body is amputated (such as a finger) there is reorganization of the primary somatosensory cortex with neurons that were previously activated by touching that finger now responding to stimulation of adjacent areas of skin..
In addition to SI, there is another representation of the body surface on the cerebral cortex - the secondary somatosensory cortex (SII) which is in Brodmann's area 40. It has inputs from both sides of the body - via SI and some less specific thalamic nuclei, but the map is less discrimintive. Some aspects of sensory experience are affected by damage to these areas.
|