A: Reflection <-> Refraction
|
| HumanPhysiology.academy |
home |
|
| |
Functional Anatomy of the eye:
|
Accomodation of the eye 1:
|
Accomodation of the eye 2:
|
Accomodation of the eye 3: Presbyopia
|
||||||
Major Refraction Anomalies: Myopia and Hyperopia.
|
Astigmatism:
|
Cataract:
|
Intra-ocular pressure and Glaucoom:
|
||||||||||
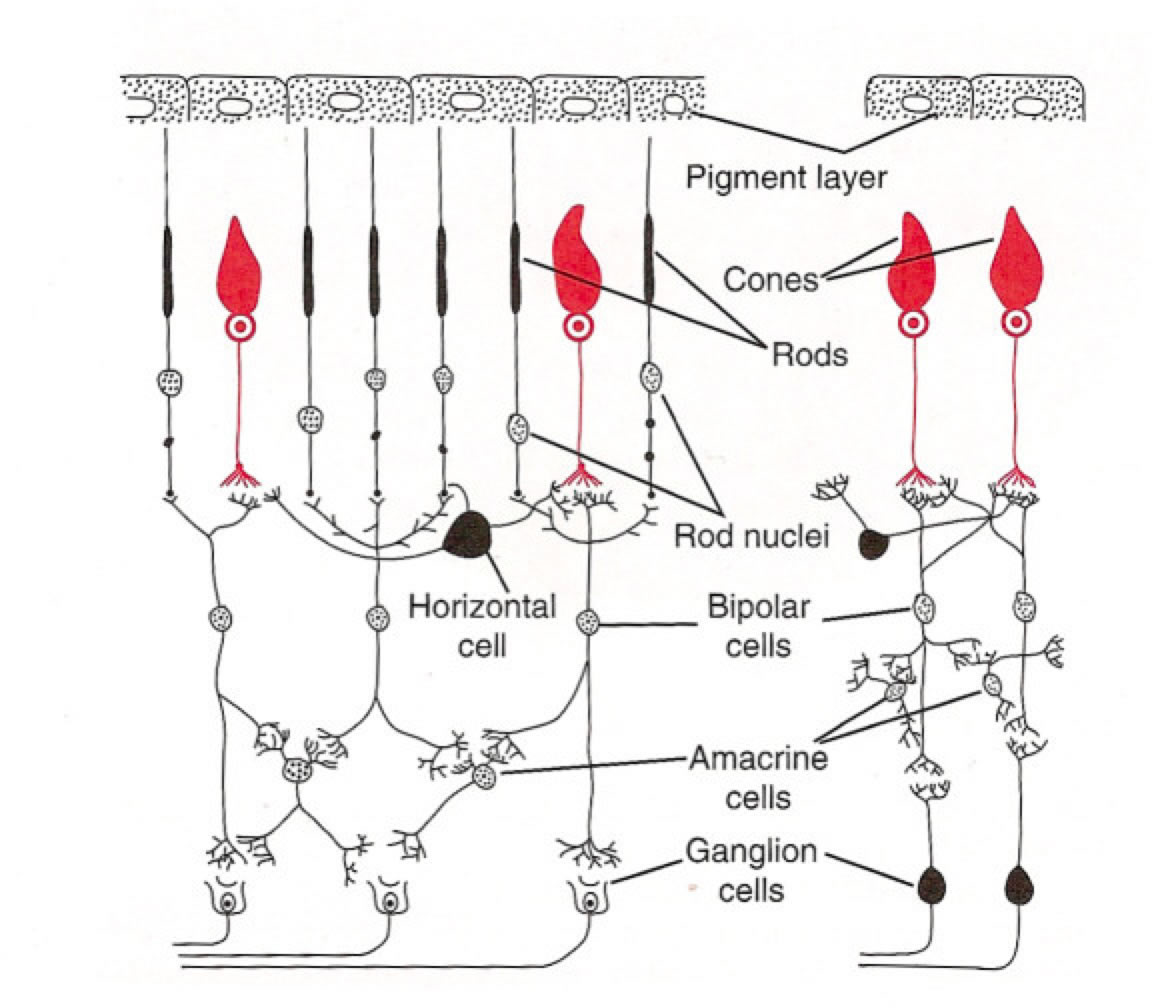
The Retina
|
The Photoreceptors
|
The Retina
|
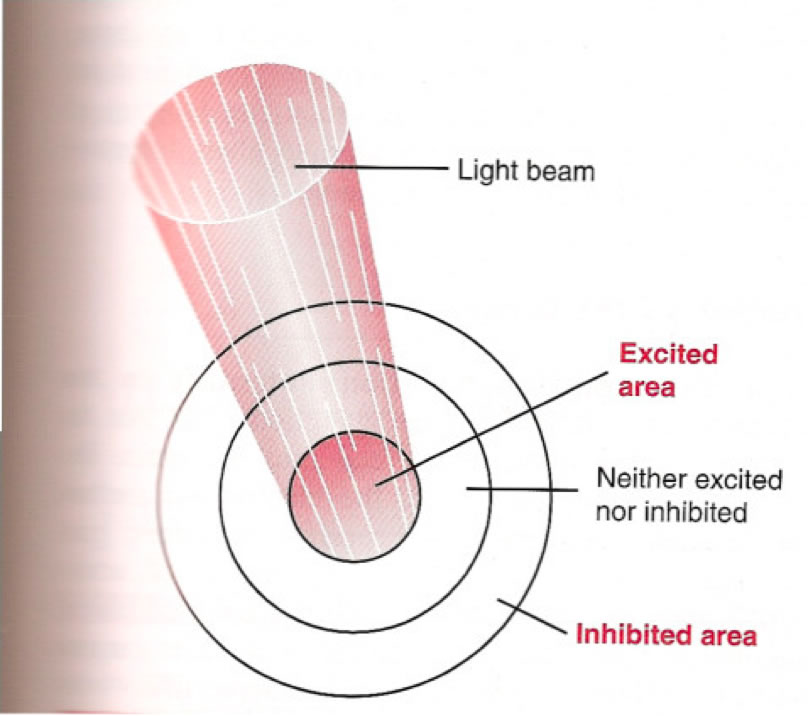
Lateral Inhibition:
|
The Iris and the Pupil:
|
||||||
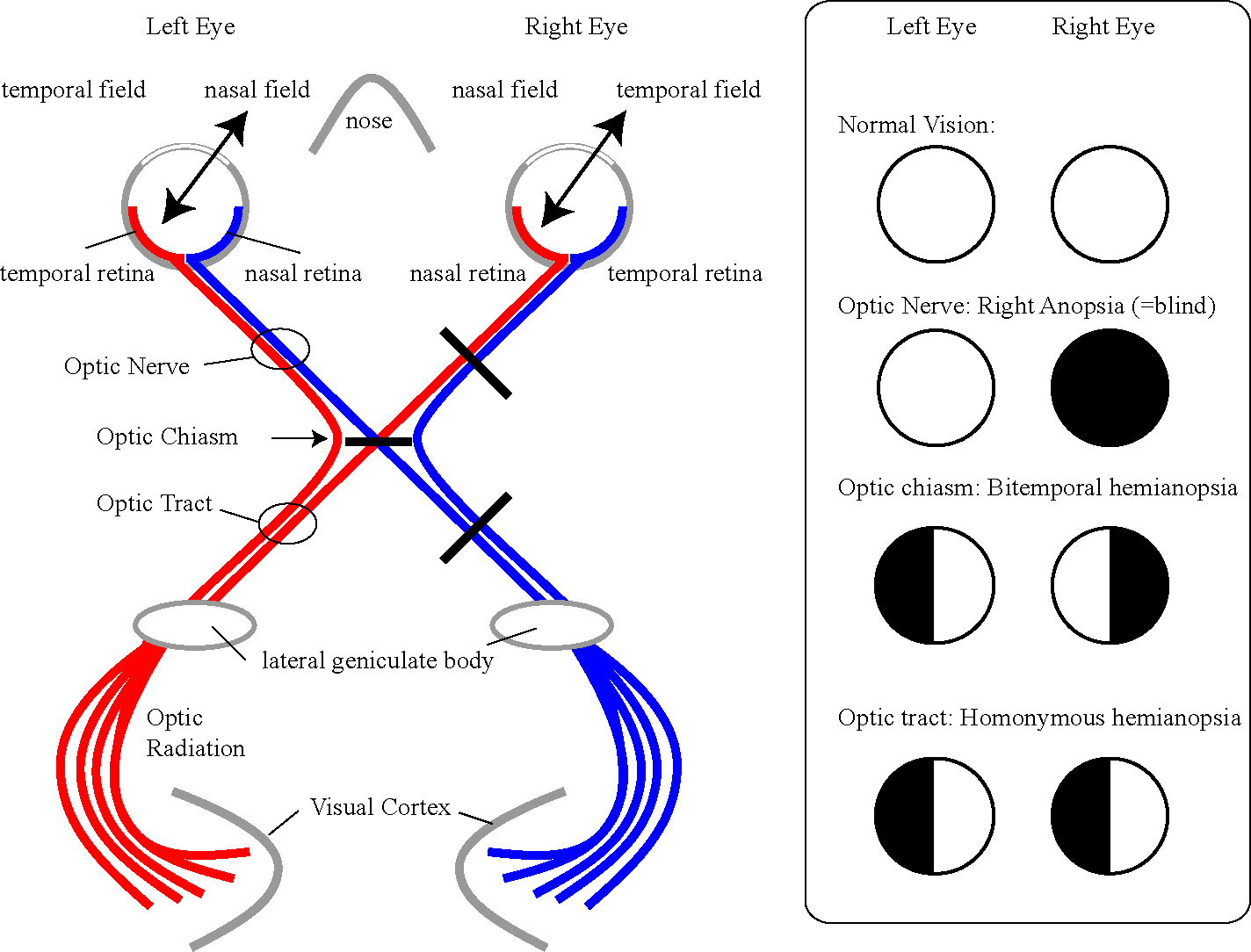
The Visual Pathways
|
|||||||
© HumanPhysiology.academy 2014